Healthy weight
Healthy weight overview
Obesity is a global and complex public health concern. It is associated with reduced life expectancy and is a risk factor for a range of chronic diseases, including cardiovascular disease, type 2 diabetes, cancer, liver, and respiratory disease, and can also impact on mental health, (OHID – Obesity profile May 2025).
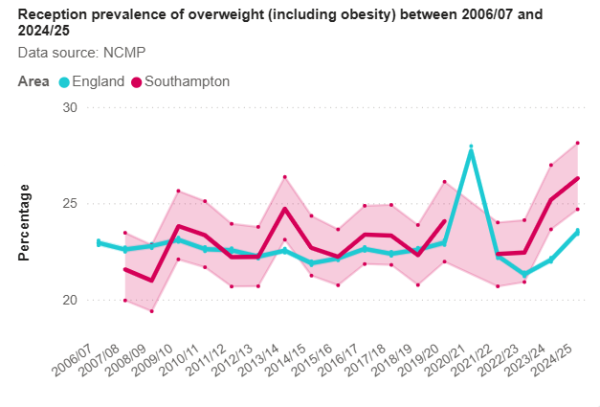
In Southampton, in 2024/25, the percentage of children in Reception Year who are overweight (including obesity), was 26.3%, significantly higher than the England average of 23.5%.
In Southampton in 2024/25, 37.9% children leaving primary school are overweight including obesity, worse but not significantly so than the England average of 36.2%.
24.9% of adults in Southampton, in 2023/24 24.9% were considered obese with a body mass index (BMI) of over 30kg/m2. Lower but not significantly when compared to the England average of 26.5%.
NCMP dashboard
Visualisation
Measuring healthy weight and obesity in Southampton
 There are several ways to measure healthy weight and obesity in the population. In children data is collected by the National Child Measurement Programme (NCMP), which uses a standardised measure to assess all children when they start and leave primary school. The NCMP measures the height and weight of children at reception (Year R) aged 4 to 5 and in their final year (Year 6) aged 10 to 11 years. Children’s Body Mass Index (BMI) is standardised for their age and sex by comparing against a recognised standard.
There are several ways to measure healthy weight and obesity in the population. In children data is collected by the National Child Measurement Programme (NCMP), which uses a standardised measure to assess all children when they start and leave primary school. The NCMP measures the height and weight of children at reception (Year R) aged 4 to 5 and in their final year (Year 6) aged 10 to 11 years. Children’s Body Mass Index (BMI) is standardised for their age and sex by comparing against a recognised standard.
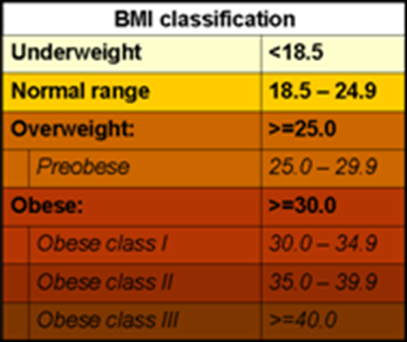
In adults, the most commonly used measure is by BMI, a simple index to classify overweight and obesity. It is defined as the weight in kilograms divided by the square of the height in metres (kg/m2).
BMI provides the most useful population-level measure of overweight and obesity, as it is the same for both sexes and for all ages of adults. However, it should be considered as a rough guide because it may not correspond to the same body fat percentage in different individuals.
More information can be found in the healthy weight dashboard below and in the resources section.
NCMP dashboard
Visualisation
Childhood obesity
 Childhood obesity is one of the most serious public health challenges of the 21st century. The World Health Organisation suggests that overweight and obese children are likely to stay obese into adulthood and more likely to develop non-communicable diseases like diabetes and cardiovascular diseases at a younger age. Overweight and obesity, as well as their related diseases, are largely preventable. Prevention of childhood obesity therefore needs to be a high priority.
Childhood obesity is one of the most serious public health challenges of the 21st century. The World Health Organisation suggests that overweight and obese children are likely to stay obese into adulthood and more likely to develop non-communicable diseases like diabetes and cardiovascular diseases at a younger age. Overweight and obesity, as well as their related diseases, are largely preventable. Prevention of childhood obesity therefore needs to be a high priority.
Data on childhood weight is taken from the NCMP, which covers children in Reception Year (aged 4 to 5 years), also known as Year R, and Year 6 (children aged 10 to 11 years) in mainstream state-maintained schools and measures children to check their weight. NCMP data enables local areas to plan services to tackle child obesity and monitor progress. For more information on defining the categories see the NHS Digital NCMP website.
In Southampton, in 2024/25, the percentage of children in Reception Year who are overweight (including obesity), was 26.3%, significantly higher than the England average of 23.5%.
72.9% are healthy weight, significantly lower than the England average of 75.4%. In Southampton 0.8% are underweight statistically similar to the England average of 1.1%.
The gap in data for 2020/21 is due to the Coronavirus pandemic when data was not collected in schools due to school closures. Nationally, increases in child obesity and severe obesity prevalence in 2020 to 2021, follow the COVID-19 pandemic which resulted in school closures and other public health measures. More data is needed to know whether this is a long-term increase. (OHID - NCMP changes in the prevalence of child obesity between 2019 to 2020 and 2020 to 2021).
During the same period in Southampton 37.9% of Year 6 children are overweight including obese, significantly similar to the England average (36.2%).
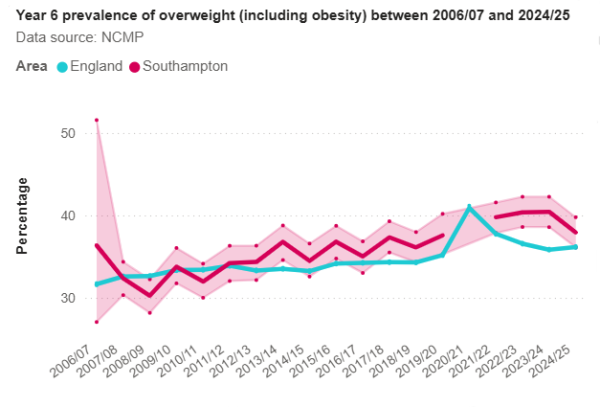 The percentage of Year 6 children who are healthy weight (61.0%) are healthy weight, significantly similar to the England average of 62,2%. In Southampton, in the same period, 1.1% are underweight, similar to the England average of 1.6%.
The percentage of Year 6 children who are healthy weight (61.0%) are healthy weight, significantly similar to the England average of 62,2%. In Southampton, in the same period, 1.1% are underweight, similar to the England average of 1.6%.
Looking at sub city areas, wards in Southampton by NCMP school weight measurements for three years between 2017-18-2019/20 and 2022/23-2024/25, the prevalence range (highest and lowest) for Reception Year by BMI category are:
- Obesity (including severe obesity) - Highest ward is Millbrook 16.0%. The lowest ward is Bassett 6.3%, both significantly different to Southampton average of 11.0%
- Overweight (including obesity) - Highest ward is Millbrook 31.0%. The lowest ward is Bassett 17.5%, both significantly different to Southampton average of 24.7%
The bullets below show the highest and lowest wards for Year 6 by BMI category for the same three year period:
- Obesity (including severe obesity) - Highest ward is Millbrook 30.2%. The lowest ward is Portswood 20.4%, with a Southampton average of 25.6%
- Overweight (including obesity) - Highest ward is Millbrook 46.0%. The lowest ward is Portswood 31.5%, followed by Shirley with 32.5%, all three wards significantly different to Southampton average of 39.6%
More information and charts for wards are available in the NCMP dashboard below or in the resources section.
NCMP dashboard
Visualisation
Linked analysis for child weight
 Analysis linking individual children’s weight recorded in Year R with that recorded for Year 6, gives an insight into childhood obesity patterns in Southampton.
Analysis linking individual children’s weight recorded in Year R with that recorded for Year 6, gives an insight into childhood obesity patterns in Southampton.
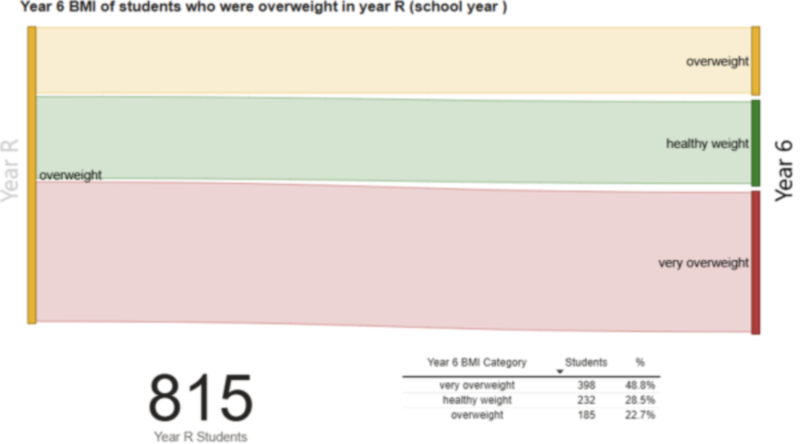
Looking at the group of children who were overweight in the three year period 2022/23 to 2024/5, Year R just under half of these (48.8%) became very overweight by the time they were in Year 6. This is 815 Year 6 children. Of those children 28.5% who were overweight became healthy weight.
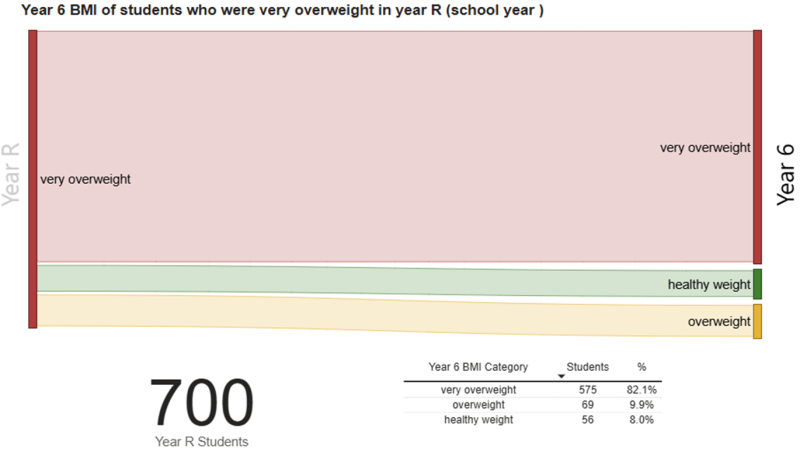
Looking at the children who are very overweight in Year R, 700 Year 6 children measured in the 3-year period 2022/23 to 2024/25 were very overweight. Of these children 82.1% of them were still very overweight in Year 6 and 92.0% of them had excess weight by the time they were in Year 6.
 In the period 2022/23 to 2024/25 (pooled), 1,723 Year 6 children measured were very overweight and 43.5% of them were a healthy weight when they were measured in Year R.
In the period 2022/23 to 2024/25 (pooled), 1,723 Year 6 children measured were very overweight and 43.5% of them were a healthy weight when they were measured in Year R.
While Year R obesity is a predictive factor for obesity in Year 6, interventions targeted at obese children in Year R will only have the potential to reduce Year 6 obesity by a maximum of one third (as two thirds of obese Year 6 children were not obese in Year R).
Healthy weight in Year R is less prevalent in the more deprived quintile (72.6%) than the least deprived quintile (77.8%). This shows a strong relationship between Year R heathy weight and deprivation.
Healthy weight in Year 6 children is statistically significantly less prevalent in the most deprived quintile (55.7%) than the least deprived quintile (67.4%) and shows a very strong relationship between Year 6 healthy weight and deprivation, (stronger than that for year R).
More information on the linked analysis is available in the Child growth report for 2025 available below and in the resources section.
NCMP dashboard
Visualisation
Child growth report December 2025
pdf | 16.2 MB | 22.12.2025
Adult weight and obesity
For adults, overweight and obesity are significant health issues across the life course and into old age. Carrying excess weight can have significant implications for an individual’s physical and mental health. There isn’t a single intervention that can tackle obesity on its own, at population or at an individual level. Causes of obesity are multi-factorial, including biological, physiological, psycho-social, behavioural and environmental factors.
Being overweight or obese is linked to a wide range of diseases, most commonly:
- type 2 diabetes
- hypertension
- some cancers
- heart disease
- stroke
- liver disease
Obesity can also be associated with poor psychological health, emotional health and poor sleep. Obese adults may also be more likely to suffer from stigma which may impact on their self-esteem.
 In Southampton, in 2023/24, it is estimated that 24.9% of adults aged 18 and over classified as obese (around 64,600 adults), higher but not significantly to England (26.5%). Adults are classified as obese if their BMI greater than or equal to 30kg/m². (OHID Fingertips Obesity profile)
In Southampton, in 2023/24, it is estimated that 24.9% of adults aged 18 and over classified as obese (around 64,600 adults), higher but not significantly to England (26.5%). Adults are classified as obese if their BMI greater than or equal to 30kg/m². (OHID Fingertips Obesity profile)
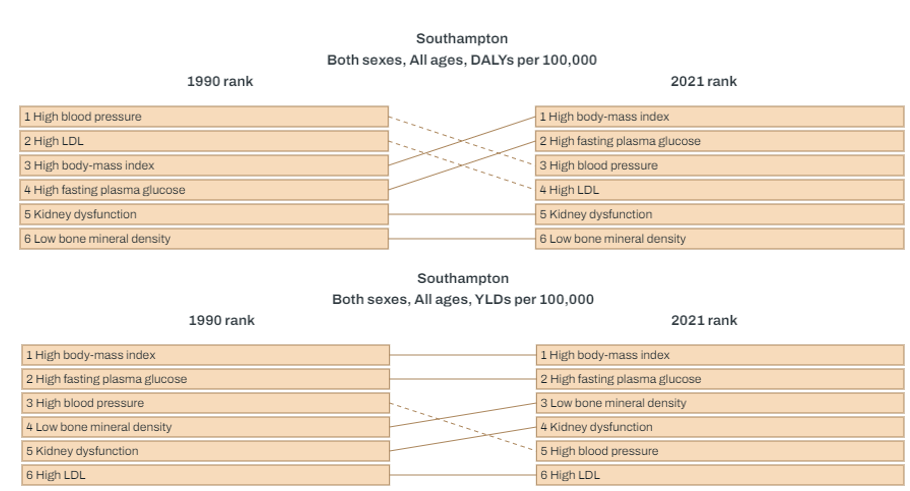
The Global Burden of Disease illustrates risk factors for mortality and poor health in Southampton and shows that high BMI feature as the third highest metabolic risk factors for Disability Adjusted Life Years Lost (DALYs) and the top metabolic risk factor for Years Lived with Disability (YLD) i.e. years of life lived with short-term or long-term health loss.
In July 2021 the Department of Health and Social Care introduced a new programme called the NHS Digital Weight Management Programme. This is to help overweight and obese adults with weight management and can be accessed with a referral from GP and primary care teams for those with a diagnosis of either diabetes, high blood pressure or both.
More information can be found in the healthy weight dashboard below and in the resources section.
Physical activity
Regular physical activity provides a range of physical, mental and social benefits, many of which are increasing issues for individuals, communities and society. These include:
- reducing the risk of and helping manage many long-term conditions, for instance type 2 diabetes and cardiovascular disease
- helping manage existing conditions
- ensuring good musculoskeletal health
- developing and maintaining physical and mental function and independence
- supporting social inclusion
- helping maintain a healthy weight
- reducing inequalities for people with long-term conditions
According to national guidelines, from the UK Chief Medical Officer (CMO), children aged 5 to 18 years should be aiming to do an average of at least 60 minutes of moderate to vigorous intensity physical activity a day across the week. Children who do less than 30 minutes a day are defined as less active, while those that do between 30 and 59 minutes are fairly active. The guidelines include activities that develop movement skills, reduce inactivity and increase muscle and bone strength.
More information is available on the physical activity page.
Physical activity dashboard
Visualisation
Tackling obesity
The NHS 10 year health plan aims to reduce the prevalence of obesity in England with restrictions on advertising “junk” food to children and embracing new weight loss medication for adults. The plan also includes expanding free school meals to all children with a parent in receipt of Universal Credit.
Resources
NCMP dashboard
The NCMP dashboard which includes benchmarking against statistical neighbours and trends over time for children’s weights from the National Child Measurement Programme (NCMP). Analysis is also included at sub-city levels and by deprivation.
NCMP dashboard
Visualisation
Physical activity dashboard
The physical activity dashboard presents a range of data regarding physical activity, to provide intelligence to help drive strategic decision making, such as the Southampton Physical Activity and Sport Strategy and Cycling Southampton. Analysis includes benchmarking against statistical neighbours and trends over time. Some indicators include analysis at a sub-city level.
Physical activity dashboard
Visualisation
Child Growth Report
Childhood obesity linked analysis of changes in weight status in Southampton between Reception year (4-5 year olds) and Year 6 (10-11 year olds) and child growth.
Child growth report December 2025
pdf | 16.2 MB | 22.12.2025
OHID National Child Measurement Programme (NCMP): Child height in England - February 2025
This slide set presents data for England on the patterns and trends in average (mean) height of children age 5 years and 11 years and the prevalence of short stature among children in reception (age 4 to 5 years) and year 6 (age 10 to 11 years).
OHID National Child Measurement Programme: Child height in England February 2025
pdf | 279.8 KB | 05.02.2025
Food environment analysis
Analysis of the food environment and location of fast-food premises and supermarkets in Southampton
Food Environment Presentation 2024
pdf | 4.0 MB | 27.11.2024
Southampton Strategic Assessment - National Child Measurement Programme
Report for Southampton scrutiny panel on using the NCMP data collected in our schools, the adult national Active People Survey and all age Health Survey for England to investigate children’s weight in Southampton.
Scrutiny NCMP intelligence
2017 PHAR: Childhood Obesity
Childhood obesity is a serious problem confronting both the current generation and also future generations, since the consequences of childhood obesity impact both on the individuals affected, and also on the wider society as we battle to make our stretched healthcare resources work effectively. Obesity harms children’s physical and emotional health in their childhood and is likely to go on to harm their adult health, cutting short lives and placing further strain on our health services. There are things that everyone can do to improve the situation – this is a problem that will need the coordinated actions of central and local governments, schools, food producers and providers, employers, and not least parents and children.
2017 PHAR: Childhood Obesity
OHID Fingertips – Obesity profile
This profile presents the latest available data to help understand and monitor the patterns and trends in obesity, physical activity and nutrition at national, regional, and local levels in England.
OHID Fingertips – Obesity, physical activity and nutrition profile
Dataset
NHS England – Fit for the future: 10 year health plan for England
The 10 year health plan for England aims to reinvent the health service through three main shifts: moving care from hospitals to communities, from analogue to digital and from treating sickness to prevention.
NHS England – Fit for the future: 10 year health plan for England
Report
NHS England - National Child Measurement Programme
This report presents the findings from the 2024 to 2025 National Child Measurement Programme (NCMP) showing the latest patterns and trends in child body mass index (BMI) category for children in reception (aged 4 to 5 years) and year 6 (aged 10 to 11 years) by age, sex, ethnic group, deprivation, region and local authority.
OHID - National Child Measurement Programme (NCMP) annual report, academic year 2024 to 2025, England
Website
World Health Organization - Obesity
Overweight and obesity are defined as abnormal or excessive fat accumulation that presents a risk to health. A body mass index (BMI) over 25 is considered overweight, and over 30 is obese. The issue has grown to epidemic proportions, with over 4 million people dying each year as a result of being overweight or obese in 2017 according to the global burden of disease.
World Health Organization - Health topic: Obesity
Website
IHME – Global burden of disease
The Global Burden of Disease (GBD) study provides a comprehensive picture of mortality and disability across countries, time, age, and sex. It quantifies health loss from hundreds of diseases, injuries, and risk factors, so that health systems can be improved and disparities eliminated.
IHME – Global burden of disease
Visualisation
OHID - Excess Weight and COVID-19
This report provides evidence-based insights on the relationship between excess weight and COVID-19. Evidence has been brought together from UK and international studies published during the pandemic. These have been identified using a pragmatic methodology; the report is not a systematic review. Findings have been contextualised with information on the prevalence, causes, and risks of excess weight. Information on food and drink purchases and physical activity during lockdown is also included.
OHID – Excess weight and COVID-19
Report
Last updated: 27 February 2026