Respiratory
 What is respiratory disease?
What is respiratory disease?
Respiratory diseases affect the lungs and respiratory system. The most common respiratory diseases are asthma, COPD (Chronic obstructive pulmonary disease) and lung diseases. Risks to respiratory diseases can include allergies, smoking, childhood respiratory infections and air pollution. NHS England Respiratory disease states respiratory disease affects one in five people and is the 3rd biggest cause of death in England. Hospital admissions have risen for lung disease over the past 7 years at three times the rate of general admissions. The most deprived areas are at higher risk of respiratory diseases as they tend to have higher smoking rates, high levels of air pollution, poor housing conditions and exposure to occupational hazards.
The Global Burden of Disease (GBD) states in 2019, Chronic respiratory diseases ranked 3rd highest cause of deaths in all ages with a rate of 67.1 per 100,000 in Southampton. This is the same rank as it was in 1990. Respiratory infections and tuberculosis are ranked 5th highest cause of death for all ages in 2019 with a rate of 47.2 per 100,000.
In 2019, Asthma was ranked 10th highest for years of life lived with disability (YLD) with a rate of 382.6 YLD per 100,000 for all ages, a decrease of 42.1% since 1990. COPD was ranked 12th highest with a rate of 331.8 YLD per 100,000.
More information is available in the Respiratory dashboard below or in the resources section.
Respiratory dashboard
Visualisation
Risks
There are many risks that are associated with respiratory diseases. Some risks are unavoidable such as genetics and allergies. Respiratory diseases are more likely to affect older people. There are modifiable risks such as smoking and environmental risks like air pollution and occupational chemicals, dust and fumes.
Smoking and second-hand smoke is one of the biggest risks for respiratory diseases. In Southampton in 2022, 13.2% of people smoke, compared with 12.7% in England and 10.5% in Hampshire. More males smoke than females and people who smoke are more likely to be between the ages of 25 and 44. Amongst men smoking peaks between the ages of 35 and 39 years (3,530 registered patients). Amongst females smoking peaks between the ages of 30 and 34 years (2,579 registered patients).
In Southampton, 25.3% of registered patients who smoke live in the 20% most deprived areas compared to just 11.1% of registered patients in the 20% least deprived areas.
In terms of wards, Thornhill has more than 1 in 4 registered patients who smoke (25.8%) and is a more deprived ward. Whereas Basset, a more affluent area, has only 14.2% of registered patients who smoke. Smoking when pregnant increases the risk of complications in pregnancy and birth. 9.7% of those that are pregnant are smoking at time of delivery in 2021/22. This percentage gives Southampton the 6th highest prevalence amongst its comparators and is also statistically similar to England (9.1%). For more information on smoking see the smoking page.
People with obesity are at increased risk of respiratory diseases such as asthma. In 2021/22, 67.0% of adults (18+) were classified as overweight or obese, the 2nd worst among Southampton’s 12 Office for National Statistics (ONS) comparator groups and higher than England (63.8%). Southampton’s trend has been slowly increasing overall along with national rates since 2015/16.
Frequent lower respiratory infection during childhood and poor lung development (pre-birth) are also risks for developing respiratory diseases in the future. In 2020/21, there were 62.1 per 100,000 emergency admissions for Southampton children under 19 with lower respiratory tract infections (LRTI), lower, but not significantly, than England (76.3). For more information see NHS Digital website on LRTIs.
In Southampton, 2021/22, there were 456.5 per 10,000 Admissions for LRTI in infants under 1 year old , the 2nd lowest against comparators and significantly lower than England (707.1).
Air pollution is an issue within Southampton due to the busy road network and the port but has improved over time. Southampton’s annual concentration of fine particulate matter (PM2.5) at an area level has decreased from 11.2 micrograms per cubic metre (µg/m3) in 2018 to 8.5 µg/m3 in 2020 during the pandemic. It has continued to decrease at a faster rate than England in 2021 to 7.8 µg/m3. New national legislation and limits on emissions may have also impacted on the reduction of air pollutions. Further post pandemic data will help explore this.
For Southampton, the under 75 mortality rate from respiratory diseases considered preventable was 23.1 per 100,000 in 2021, significantly higher than England (15.6) and 4th worst against ONS. The mortality rate considered preventable between males and females is similar (22.9 and 23.1 respectively) and both higher than England. However, female mortality rate considered preventable is the 2nd worst amongst ONS comparators, whereas males is the 6th worst.
More information is available in the Respiratory dashboard below or in the resources section at the bottom of the page.
Respiratory dashboard
Visualisation
Impact of respiratory disease on life expectancy
 In 2018-20, male life expectancy was 78.3 years; significantly lower than England (79.4 years), and 5th lowest out of 12 in Southampton’s ONS comparator group. For females, life expectancy at birth was improving (82.5 years); significantly lower than England (83.1 years) and the 7th lowest amongst Southampton’s 12 ONS comparators group.
In 2018-20, male life expectancy was 78.3 years; significantly lower than England (79.4 years), and 5th lowest out of 12 in Southampton’s ONS comparator group. For females, life expectancy at birth was improving (82.5 years); significantly lower than England (83.1 years) and the 7th lowest amongst Southampton’s 12 ONS comparators group.
The life expectancy at birth gap between the most deprived 20% of Southampton to the least deprived 20%, is 7.8 years for men and 3.4 years for women (2019-21).
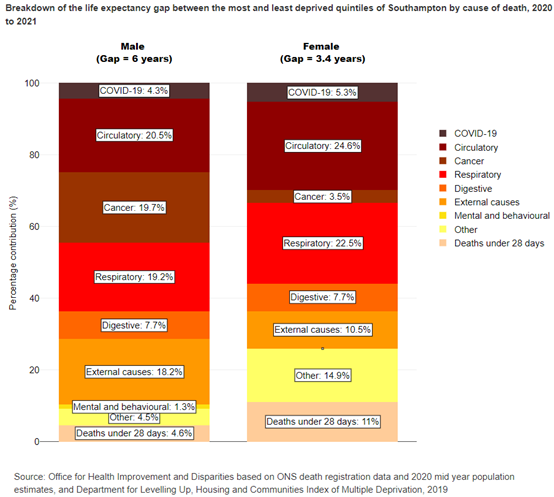
The Office for Health Improvement and Disparities (OHID) inequalities segment tool indicates that in 2020 to 2021, respiratory deaths contribute 18.7% of the gap in male life expectancy compared to England, the 3rd largest group. On closer inspection, the largest cause is chronic lower respiratory disease, contributing 0.25 years to the gap in life expectancy, followed by lung cancer and other circulatory both contributing 0.18 years. For females, respiratory diseases contribute 23.9% of the gap in life expectancy compared to England, the 2nd highest group. More detailed analysis shows chronic lower respiratory diseases is the 3rd largest cause of the gap in female life expectancy (0.17 years). COVID-19 contributed 4.3% to the gap in male life expectancy and 5.3% to the gap for females.
When look at the gap in life expectancy between the most and least deprived quintiles of Southampton, respiratory contributed to 19.2% of the gap in life expectancy for males, the 3rd highest, and 22.5% for females, the 2nd highest. Further analysis shows chronic lower respiratory diseases is the largest cause for the life expectancy gap in both male and females with a contribution of 0.91 years and 0.63 years respectively.
For more information see the life expectancy page.
Respiratory dashboard
Visualisation
Mortality and years of life lost (YLL) from respiratory disease
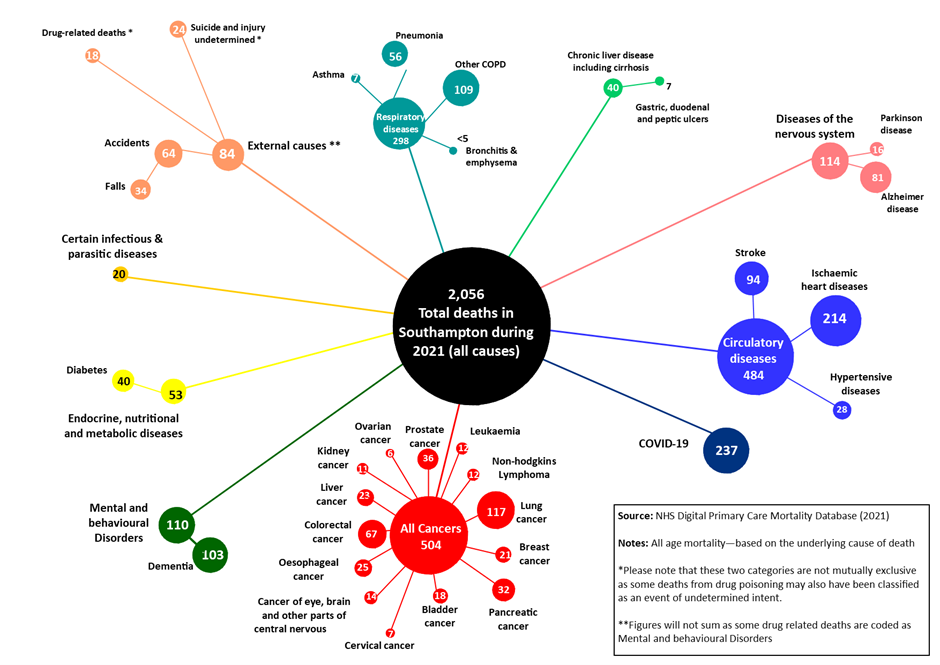 In 2021, of the 2,056 deaths registered in Southampton’s resident population, 298 (14.5%) were due to respiratory diseases - the 3rd highest cause of death. The largest subgroup was “Other COPD” with 109 deaths, 5.3% of all deaths but 36.5% of respiratory deaths. Pneumonia was the second largest subgroup with 56 deaths, 2.7% of all deaths and 18.8% of respiratory deaths. There were 7 deaths from asthma and less than 5 for bronchitis and emphysema. There was a total of 31,357 years of life lost in Southampton in 2019-2021 (pooled). Of these, 1,832 years (5.8%) were due to respiratory diseases. Breaking this down into specific respiratory diseases, 49.6% (909) of total respiratory YLL were “Other COPD”, 28.3% (518) due to pneumonia, 2.9% (53) from bronchitis and emphysema and 3.8% (70) to asthma.
In 2021, of the 2,056 deaths registered in Southampton’s resident population, 298 (14.5%) were due to respiratory diseases - the 3rd highest cause of death. The largest subgroup was “Other COPD” with 109 deaths, 5.3% of all deaths but 36.5% of respiratory deaths. Pneumonia was the second largest subgroup with 56 deaths, 2.7% of all deaths and 18.8% of respiratory deaths. There were 7 deaths from asthma and less than 5 for bronchitis and emphysema. There was a total of 31,357 years of life lost in Southampton in 2019-2021 (pooled). Of these, 1,832 years (5.8%) were due to respiratory diseases. Breaking this down into specific respiratory diseases, 49.6% (909) of total respiratory YLL were “Other COPD”, 28.3% (518) due to pneumonia, 2.9% (53) from bronchitis and emphysema and 3.8% (70) to asthma.
For more information and a visualisation looking at Year of Life Lost over time is available on the Mortality page.
Respiratory dashboard
Visualisation
Respiratory disease in Southampton
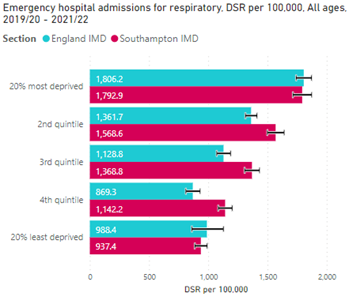 Since 2017/18 – 2019/20 the rate of emergency admissions in Southampton has been decreasing. There was a total of 8,945 emergency hospital admissions for respiratory diseases in Southampton in 2019/20 to 2021/22, a DSR of 1,346.5 per 100,000 population. Babies and young children aged 0-4 had the highest number of emergency admissions (990) however this is most likely due to lower respiratory tract infections (LRTI) being common in babies. Emergency admissions start to increase considerably at ages 60-64 with people aged 75 to 79 years have the 2nd highest amount of emergency admissions (855) compared to ages 10 to 14 who have the lowest (120). Coxford had the highest DSR for emergency respiratory admissions (1,817.0 per 100,000 population) while Freemantle had the lowest (1,105.6 per 100,000). Using Southampton deprivation quintiles, the 20% most deprived areas in Southampton had a DSR of 1,792.9 per 100,000 population. This decreases across the quintiles as affluence increases to 937.4 in the 20% least deprived areas – nearly two times lower. With an R2 value of 0.97, there shows a very high correlation between deprivation and respiratory admissions.
Since 2017/18 – 2019/20 the rate of emergency admissions in Southampton has been decreasing. There was a total of 8,945 emergency hospital admissions for respiratory diseases in Southampton in 2019/20 to 2021/22, a DSR of 1,346.5 per 100,000 population. Babies and young children aged 0-4 had the highest number of emergency admissions (990) however this is most likely due to lower respiratory tract infections (LRTI) being common in babies. Emergency admissions start to increase considerably at ages 60-64 with people aged 75 to 79 years have the 2nd highest amount of emergency admissions (855) compared to ages 10 to 14 who have the lowest (120). Coxford had the highest DSR for emergency respiratory admissions (1,817.0 per 100,000 population) while Freemantle had the lowest (1,105.6 per 100,000). Using Southampton deprivation quintiles, the 20% most deprived areas in Southampton had a DSR of 1,792.9 per 100,000 population. This decreases across the quintiles as affluence increases to 937.4 in the 20% least deprived areas – nearly two times lower. With an R2 value of 0.97, there shows a very high correlation between deprivation and respiratory admissions.
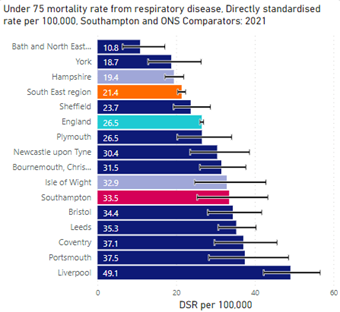
Southampton’s under 75 years mortality rate from respiratory disease in 2021 was 33.5 per 100,000, the 6th highest compared to our ONS comparators and higher, but not significantly, than England (26.5). Males had a higher mortality rate of 36.2 per 100,000 in 2021 and the rate for females was 30.7 per 100,000. However, Southampton has the 3rd highest mortality rate for females compared to ONS comparators.
 The 20% most deprived areas of Southampton (by England IMD) had the highest under 75 mortality rate of 66.7 per 100,000 for 2019-2021, whilst the 4th quintile had the lowest, 13.1 per 100,000.
The 20% most deprived areas of Southampton (by England IMD) had the highest under 75 mortality rate of 66.7 per 100,000 for 2019-2021, whilst the 4th quintile had the lowest, 13.1 per 100,000.
There is a strong correlation between respiratory deaths and deprivation within Southampton. More deprived areas tend to have higher smoking rates which is a high-risk factor to respiratory diseases.
Swaythling ward has the highest DSR per 100,000 for respiratory deaths between 2019-2021 of 64.2, over 3 times higher than Bassett ward which has the lowest rate of 18.9 per 100,000.
More information is available in the Respiratory dashboard below or in the resources section at the bottom of the page.
Respiratory dashboard
Visualisation
Asthma
 Asthma affects the respiratory system and is a very common long-term lung condition. Asthma often starts in childhood, however, can develop in adult too. Asthma can vary from person to person and can be managed everyday with inhalers. Environmental and lifestyle risks can trigger asthma, more information on the causes of Asthma is available on the Asthma UK website.
Asthma affects the respiratory system and is a very common long-term lung condition. Asthma often starts in childhood, however, can develop in adult too. Asthma can vary from person to person and can be managed everyday with inhalers. Environmental and lifestyle risks can trigger asthma, more information on the causes of Asthma is available on the Asthma UK website.
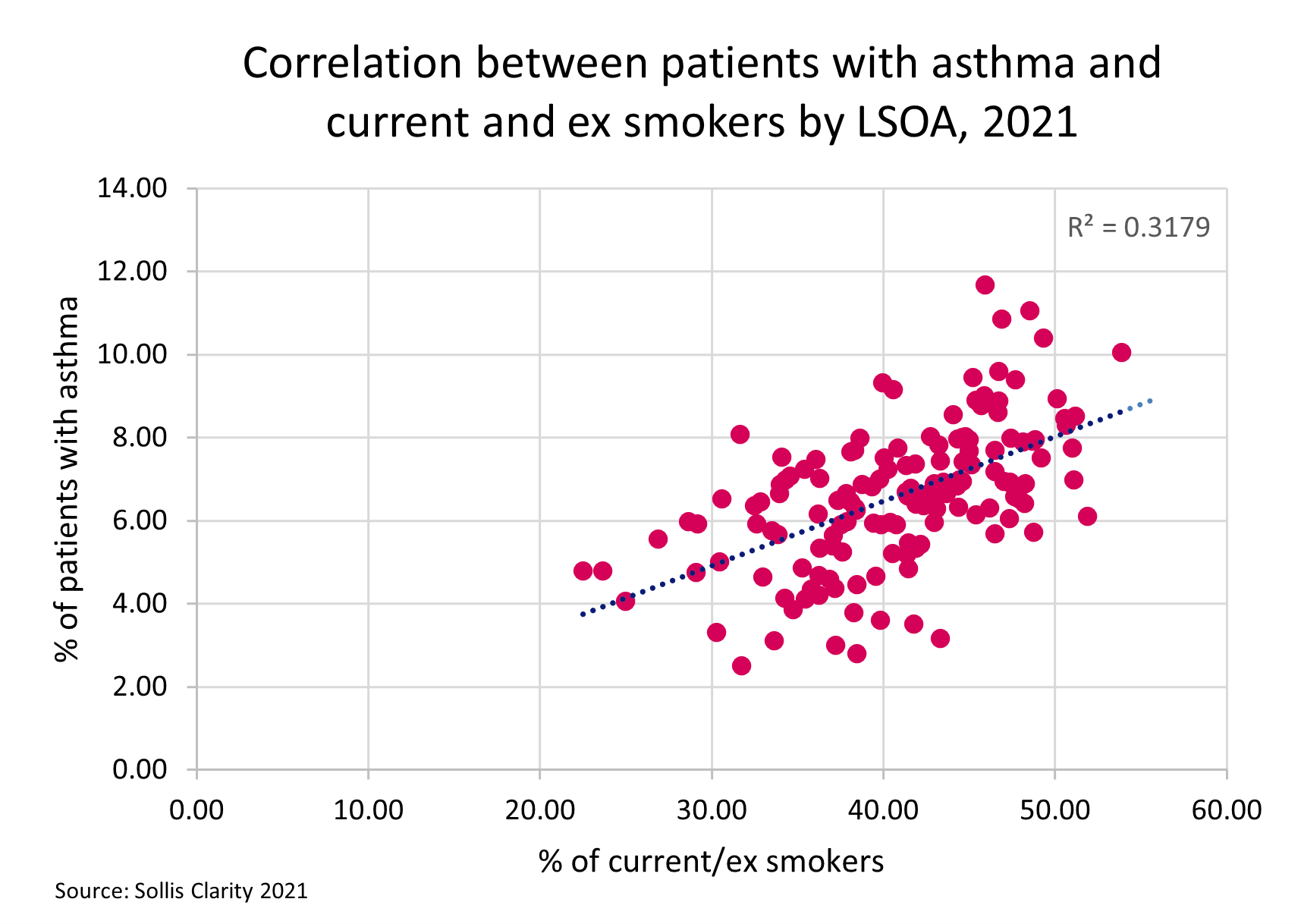
Of Southampton residents registered with a GP, 6.5% (14,553) are known to have asthma. The age band with the highest count of patients with asthma is 45 to 49 years (1,229 patients). However, the age band with the highest prevalence is 80 to 84 years (10.3%). Of all patients with asthma, 27.0% (3,926) are current smokers, 29.3% are ex-smokers and 43.7% are non-smokers.
 Analysis of GP data at LSOA neighbourhood level shows a moderate correlation between areas with high smoking or ex-smoker prevalence and those areas with a high prevalence of asthma. Southampton had 85 hospital admissions for asthma in under 19 year olds in 2021/22, a crude rate per 100,000 of 162.2, 2nd highest amongst comparators and higher, but not significantly, than England (131.5 per 100,000). Of the 85 admissions, 35 were for ages 0-9, a crude rate of 125.1 per 100,000, the 7th lowest amongst comparators and lower, but not significantly, than England’s rate (172.7). The remaining 50 admissions were in ages 10-18, a crude rate of 204.8, the highest against comparators and significantly higher than England (87.6 per 100,000). This could be due to the higher likelihood of people smoking from ages 15 to 18 years and the new use of vapes among young people.
Analysis of GP data at LSOA neighbourhood level shows a moderate correlation between areas with high smoking or ex-smoker prevalence and those areas with a high prevalence of asthma. Southampton had 85 hospital admissions for asthma in under 19 year olds in 2021/22, a crude rate per 100,000 of 162.2, 2nd highest amongst comparators and higher, but not significantly, than England (131.5 per 100,000). Of the 85 admissions, 35 were for ages 0-9, a crude rate of 125.1 per 100,000, the 7th lowest amongst comparators and lower, but not significantly, than England’s rate (172.7). The remaining 50 admissions were in ages 10-18, a crude rate of 204.8, the highest against comparators and significantly higher than England (87.6 per 100,000). This could be due to the higher likelihood of people smoking from ages 15 to 18 years and the new use of vapes among young people.
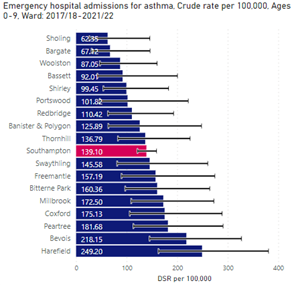
At sub-city level from 2019/20 – 2021/22, asthma admissions in ages 0-18 year olds were higher in the top two most deprived quintiles in Southampton (by England IMD). By ward, Peartree had the highest DSR of 227.8 per 100,000, 1.8 times higher than the Southampton average of 128.9 per 100,000.
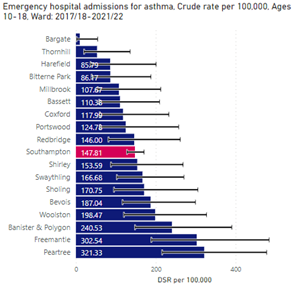 In the same pooled period, the highest admissions in ages 0-9 years were in the 20% most deprived areas of Southampton with a crude rate of 161.2 per 100,000 whereas for ages 10-18, the highest admissions were in the 2nd quintile with a crude rate of 185.1 per 100,000. Looking at the most recent 5 years pooled by ward, Peartree is the 3rd highest for asthma admissions in ages 0-9 with a crude rate of 181.7 per 100,000 and the highest for ages 10-18 with a crude rate of 321.3 per 100,000.Local deaths register data shows in 2021, there were 7 deaths with an underlying cause of asthma.
In the same pooled period, the highest admissions in ages 0-9 years were in the 20% most deprived areas of Southampton with a crude rate of 161.2 per 100,000 whereas for ages 10-18, the highest admissions were in the 2nd quintile with a crude rate of 185.1 per 100,000. Looking at the most recent 5 years pooled by ward, Peartree is the 3rd highest for asthma admissions in ages 0-9 with a crude rate of 181.7 per 100,000 and the highest for ages 10-18 with a crude rate of 321.3 per 100,000.Local deaths register data shows in 2021, there were 7 deaths with an underlying cause of asthma.
More information is available in the Respiratory dashboard below or in the resources section at the bottom of the page.
Respiratory dashboard
Visualisation
Chronic obstructive pulmonary disease (COPD)
COPD is a group of lung conditions that cause difficulty breathing. Smoking is the main cause of COPD and mainly affects middle-aged and older adults who smoke. Lung conditions include emphysema and chronic bronchitis. COPD causes permanent damage to the lungs however the condition can be treated to slow the development. For more information see the NHS - COPD website.
In Southampton, the prevalence of GP registered patients registered in 2021 with a diagnosis of COPD aged 35+ is 2.5% (5,666). The highest number of people with COPD are in the age range of 70-74 years with 927 patients however ages 80 to 84 have the highest prevalence at 15.9%. Redbridge ward has the highest prevalence at 3.9% whilst Bevois has the lowest prevalence of 1.1%.
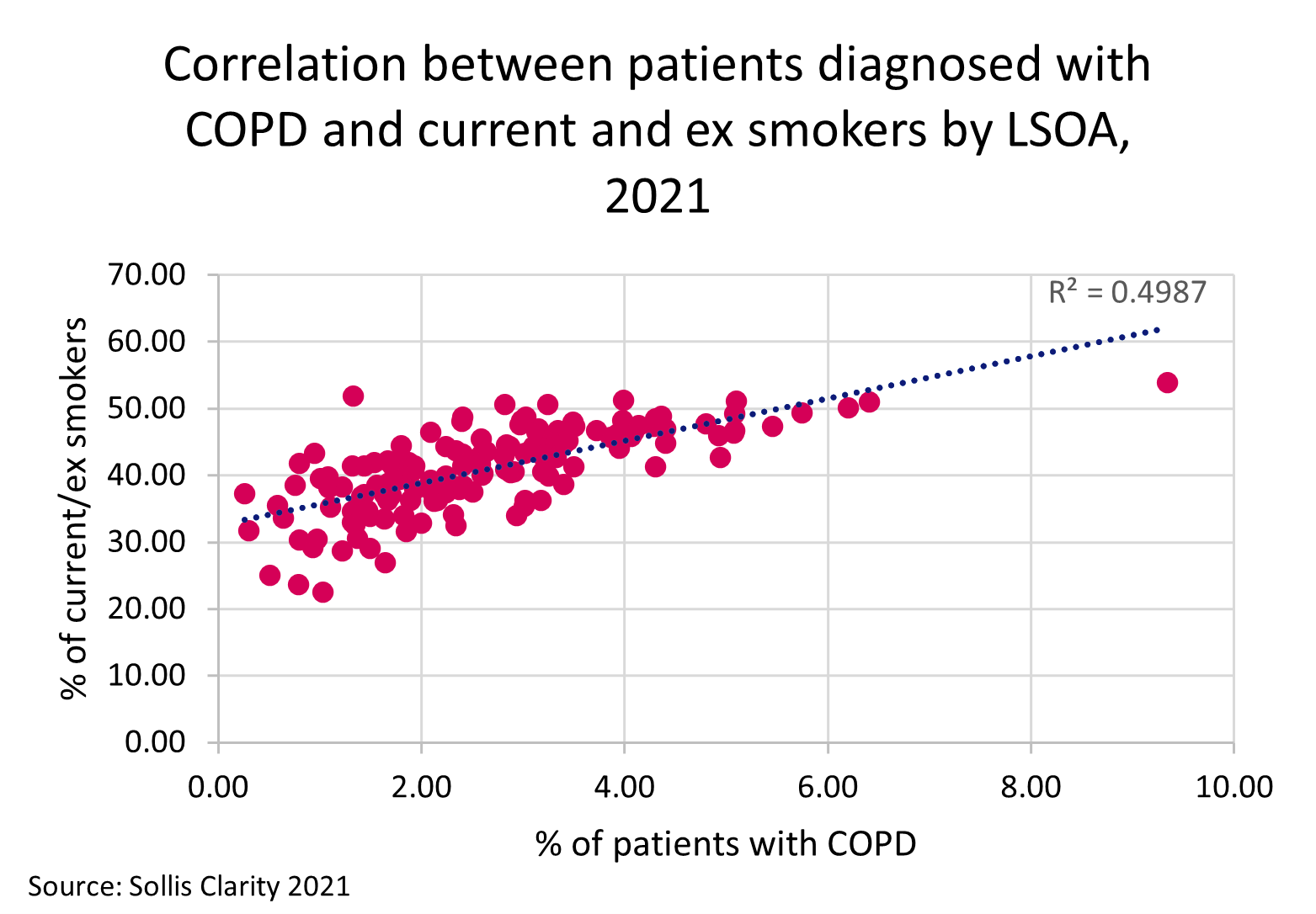
Analysis of GP data at LSOA (neighbourhood level) shows a high correlation between areas with high smoking or ex-smoker prevalence and those areas with a high prevalence of COPD. Looking specifically at those diagnosed with COPD 94.6% were ex or current smokers further highlighting the impact of smoking on COPD.
 Southampton had 725 emergency hospital admissions for COPD ages 35+ in 2019/20, a DSR of 677.0 per 100,000. This is the 3rd worst against comparators and significantly higher than England’s rate (415.1 per 100,000). Of the 725 admissions, 380 admissions were females, a DSR of 664.7 and 3rd worst amongst comparators. This is significantly higher than England and been increasing steadily since 2010/11. For males, there were 350 admissions, a DSR of 712.2 and 2nd worst amongst ONS comparators. The rate has been significantly higher than England since 2010/11.
Southampton had 725 emergency hospital admissions for COPD ages 35+ in 2019/20, a DSR of 677.0 per 100,000. This is the 3rd worst against comparators and significantly higher than England’s rate (415.1 per 100,000). Of the 725 admissions, 380 admissions were females, a DSR of 664.7 and 3rd worst amongst comparators. This is significantly higher than England and been increasing steadily since 2010/11. For males, there were 350 admissions, a DSR of 712.2 and 2nd worst amongst ONS comparators. The rate has been significantly higher than England since 2010/11.
At sub city level in 2019/20 – 2021/22, Coxford ward had the highest COPD admissions ages 35+ with a DSR of 772.8 per 100,000 although higher than the Southampton average (507.5 per 100,000) Coxford ward rate has been decreasing quicker. Portswood had the lowest crude rate of 317.6 per 100,000. Looking at admissions by England IMD in ages 35+, the R correlation value is 0.36, showing a low correlation between the rates and deprivation. However, by Southampton IMD, the R value of 0.95 shows a very high correlation. In 2021, there were 110 deaths from COPD with a DSR per 100,00 of 61.1, the 2nd worst amongst comparators and significantly higher in England’s rate (39.8 per 100,000).
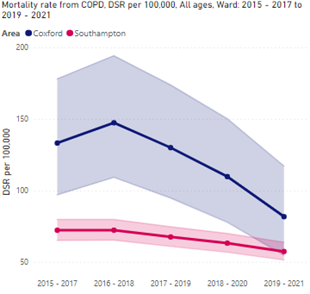 At sub city level, Coxford has the highest DSR of 81.7 per 100,000 for COPD deaths between 2019 and 2021, 1.4 times higher than the Southampton average of 57.3 per 100,000, however, this gap has been decreasing. Bassett has the lowest mortality rate of 29.2 per 100,000. Looking at COPD mortality by England IMD 2019-2021 pooled, there is a high correlation between COPD deaths and deprivation with a R value of 0.77. There is also a high correlation when looking at COPD deaths by Southampton IMD with a R value of 0.85.
At sub city level, Coxford has the highest DSR of 81.7 per 100,000 for COPD deaths between 2019 and 2021, 1.4 times higher than the Southampton average of 57.3 per 100,000, however, this gap has been decreasing. Bassett has the lowest mortality rate of 29.2 per 100,000. Looking at COPD mortality by England IMD 2019-2021 pooled, there is a high correlation between COPD deaths and deprivation with a R value of 0.77. There is also a high correlation when looking at COPD deaths by Southampton IMD with a R value of 0.85.
Bronchitis and Emphysema are types of COPD. POPPI (projecting older people population information system) predicts that in 2022, 591 people ages 65 and over will have had a long-standing health condition caused by bronchitis and emphysema in Southampton. In two years, it is predicted to rise by 3.6% (percentage increase) to 612 people. By 2040, it is predicted 758 people (28.3% percentage increase) in Southampton will have a longstanding health condition caused by bronchitis and emphysema. This shows a projected steady increase in long standing health conditions in Southampton.
More information is available in the Respiratory dashboard below or in the resources section at the bottom of the page.
Respiratory dashboard
Visualisation
Pneumonia
Pneumonia is different to asthma and COPD, as it is a chest infection that can be caught and treated. People can make a full recovery, although it can be life-threatening. It can also be caught more than once. It is more common to get pneumonia in the winter due to viral infections being easily spread and the pneumonia is often caused by a secondary bacterial infection. People who smoke are in the at-risk category, as well as babies and people over 65. More information on pneumonia is available from the Asthma and Lung UK website.
In 2019/20 – 2021/22, there were a total of 2,576 emergency admissions for pneumonia in Southampton with a DSR of 412.0 per 100,000, with 2,015 (78%) of these admissions being in ages 60+. Bevois had the highest number of admissions with a DSR of 545.2 per 100,000. GP patient data in 2021 shows Bevois is the 7th highest ward for patients who are current and ex smokers which can explain a higher number of admissions. Redbridge has the 2nd highest DSR of 520.5 per 100,000 for pneumonia admissions and also has the 2nd highest number of current and ex-smokers, further suggesting smoking as a possible contributing factor. With a R value of 0.96, there is a very high correlation between pneumonia admissions and deprivation (by England IMD).
In 2019-2021 (pooled), there were a total of 187 deaths due to pneumonia in Southampton with 81% of these deaths in ages 75+. Although Basset has the lowest pneumonia admissions DSR, it has the highest pneumonia mortality DSR of 41.1 per 100,000, 1.4 times higher than the Southampton average of 29.6 per 100,000. There is no correlation between pneumonia mortality and deprivation. The 20% least deprived areas in Southampton (by England IMD) had the highest DSR of 54.2 per 100,000. The least deprived areas tend to have an older population that have a greater affluence to age into frailty which may result in higher mortality, however there are caveats (area of least deprivation are not always where the older population live and there are many factors that go to make up the IMD overall score).
Tuberculosis is also being monitored as part of respiratory infections included in Health Protection. More information can be found on our Health Protection page.
More information is available in the Respiratory dashboard below or in the resources section.
Respiratory dashboard
Visualisation
Tuberculosis
Tuberculosis (TB) is a bacterial infection that mainly affects the lungs. It is spread through inhaling tiny droplets from coughs and sneezes of an infected person. More information is available from the NHS England Tuberculosis website. It is considered a risk factor to developing COPD. Between 2019 and 2021 (pooled), Southampton’s count of Tuberculosis incidences was 60, giving a crude rate of 7.9 per 100,000, the 4th worst against ONS comparators and local neighbours and similar to England’s rate of 7.8.
The rate between 2004-06 and 2008-10 for Southampton was lower than England, however since 2009-11 Southampton’s rate has remained higher than the national average.
More information is available in the Respiratory dashboard below or in the resources section at the bottom of the page.
Respiratory dashboard
Visualisation
COVID-19
COVID-19 is considered a respiratory illness, affecting the lungs along with other symptoms. Anyone can catch COVID-19, however if people have an underlying respiratory condition, they are considered higher risk. For more information on COVID-19 see the World Health Organization’s website.
The pandemic has affected people with existing illness in many ways. People with a pre-existing illness were more likely to experience severe outcomes from COVID-19. The impact of the move to online consultations (and the speed with which this was done) in primary care may have affected accessibility, particularly for chronic disease management. Contracting COVID-19 may have exacerbated existing illness. Due to reduced opportunities to diagnose disease early (for example though NHS health checks which were suspended across the country during earlier parts of the pandemic) and concern about potential infection or adding pressure to the NHS led some patients to stay away from healthcare meaning respiratory conditions may have not been diagnosed or treated early enough causing serious illness or death.
For more information on the impacts of COVID see the COVID impacts assessment. Available in the resources section below.
Respiratory dashboard
Visualisation
Resources
Respiratory dashboard
Respiratory diseases affect the lungs and respiratory system. This dashboard includes analysis and benchmarking against statistical neighbours and trends over time for all indicators included.
Respiratory dashboard
Visualisation
COVID-19 Impact Assessment update August 2022
Refresh of the COVID-19 Impact Assessment. This health impact assessment will be used to inform and support prioritisation within the Southampton health and wellbeing strategy.
Covid19 Impact Assessment Update August 2022
pdf | 6.1 MB | 24.08.2022
COVID-19 Impact Assessment
A COVID-19 Health Impact Assessment has been conducted to highlight emerging direct and indirect health impacts of the pandemic on people living in Southampton. This health impact assessment will be used to inform and support prioritisation of specific actions within the Southampton health and wellbeing strategy.
COVID-19 Impact Assessment
pdf | 8.2 MB | 01.12.2021
Long term conditions
Summary long term conditions prevalence in Southampton and projections of how they are expected to grow in the future.
Current and predicted chronic conditions and predicted need for help - October 2022
pdf | 14.8 MB | 26.10.2022
Health Protection Dashboard
Data from a range of Health Protection measures including Gastrointestinal infections Immunisations and childhood vaccine preventable diseases, respiratory infections, hepatitis, Sexually Transmitted Infections and HIV.
Health Protection Dashboard
Visualisation
Hampshire County Council (HCC) - Major conditions report
The major conditions report from Hampshire County Council includes information about prevalence, emergency admissions and deaths in seven major conditions: cancer, cardiovascular disease, respiratory disease, dementia, mental health, musculoskeletal conditions and chronic kidney disease.
HCC - Major conditions report
Visualisation
World Health Organization - Information on COVID-19
World Health Organization information on COVID-19. The best way to prevent and slow down transmission is to be well informed about the disease and how the virus spreads. Protect yourself and others from infection by staying at least 1 metre apart from others, wearing a properly fitted mask, and washing your hands or using an alcohol-based rub frequently. Get vaccinated when it’s your turn and follow local guidance.
World Health Organization - Coronavirus
Website
Asthma and lung UK - What is pneumonia?
Pneumonia is a type of chest infection. It affects the tiny air sacs (alveoli) in your lungs. When you have pneumonia, these air sacs get swollen and fill with fluid. This makes it harder for you to breathe.
Asthma and lung UK - What is pneumonia?
Website
NHS England - Emergency admissions for children with lower respiratory tract infections (LRTIs)
This indicator measures the number of emergency admissions to hospital of children with selected types of lower respiratory tract infections (bronchiolitis, bronchopneumonia and pneumonia). This indicator is concerned with how successfully the NHS manages to reduce avoidable emergency admissions for children with lower respiratory tract infections (LRTIs). The coronavirus (COVID-19) pandemic began to have an impact on Hospital Episode Statistics (HES) data late in the 2019/20 financial year, which continued into the 2020/21 financial year. This means we are seeing different patterns in the submitted data, for example, fewer patients being admitted to hospital, and therefore statistics which contain data from this period should be interpreted with care.
NHS England - Emergency admissions for children with lower respiratory tract infections
Website
IHME – Global Burden of Disease
The Global Burden of Disease (GBD) study provides a comprehensive picture of mortality and disability across countries, time, age, and sex. It quantifies health loss from hundreds of diseases, injuries, and risk factors, so that health systems can be improved and disparities eliminated.
IHME – Global Burden of Disease
Visualisation
Projecting Older People Population Information (POPPI)
Projecting Older People Population Information (POPPI) is a view-only system is developed by the Institute of Public Care (IPC). It is a programme designed to help explore the possible impact that demography and certain conditions may have on populations aged 65 and over.
Oxford Brookes University - Projecting Older People Population Information (POPPI)
Website
Projecting Adult Needs and Service Information (PANSI)
Projecting Adult Needs and Service Information (PANSI), sister site to POPPI, is a view-only system is developed by the Institute of Public Care (IPC). With a programme designed to help explore the possible impact that demography and certain conditions may have on populations aged 18 to 64.
Oxford Brookes University - Projecting Adult Needs and Service Information (PANSI)
Website
NHS - Chronic obstructive pulmonary disease (COPD)
Chronic obstructive pulmonary disease (COPD) is the name for a group of lung conditions that cause breathing difficulties. It includes emphysema – damage to the air sacs in the lungs, chronic bronchitis – long-term inflammation of the airways, COPD is a common condition that mainly affects middle-aged or older adults who smoke. Many people do not realise they have it. The breathing problems tend to get gradually worse over time and can limit your normal activities, although treatment can help keep the condition under control.
NHS - Chronic obstructive pulmonary disease (COPD)
Website
NHS - Pneumonia
Pneumonia is inflammation of the lungs, usually caused by an infection. Most people get better in 2 to 4 weeks, but babies, older people, and people with heart or lung conditions are at risk of getting seriously ill and may need treatment in hospital.
NHS - Pneumonia
Website
NHS - Tuberculosis (TB)
Tuberculosis (TB) is an infection that usually affects the lungs. It can be treated with antibiotics but can be serious if not treated. There's a vaccine that helps protect some people who are at risk from TB.
NHS - Tuberculosis
Website
Last updated: 03 October 2023